What palpitations actually are
A “palpitation” is the conscious awareness of a heartbeat that you normally would not feel. The sensation varies enormously from person to person — a flutter, a flip, a pause followed by a thud, a sudden gallop, a steady racing — and the words people use don’t reliably point to one specific rhythm. That’s why a tracing during the event is so much more valuable than any description.
It’s worth saying clearly: feeling your heart is not the same as something being wrong with your heart. Most palpitations come from harmless rhythms in otherwise healthy hearts.
Common causes
Premature beats — PACs and PVCs
By far the most common explanation. PACs (premature atrial contractions) and PVCs (premature ventricular contractions) are extra beats that arrive earlier than the next scheduled beat. The premature beat itself is usually weak (the heart hasn’t fully refilled), then there’s a brief pause, then the next normal beat is unusually strong — and that strong beat is what most patients actually feel. The classic description is a “skip” or a “flip-flop” in the chest.
Occasional PACs and PVCs are universal — everyone has them. They become a concern when they are very frequent (a meaningful percentage of total beats over a day), when they cluster into runs, or when they happen in a heart with weakened muscle.
Sustained arrhythmias
- Supraventricular tachycardia (SVT). A sudden onset of a fast, regular heartbeat that starts and stops in an instant.
- Atrial fibrillation (AFib). A fast, irregular, chaotic pattern. Some patients clearly feel the irregularity; others feel nothing at all.
- Ventricular tachycardia (VT). Less common, more serious. Usually causes lightheadedness or worse along with the racing sensation.
Triggers that amplify normal beats
- Stimulants — caffeine, nicotine, certain decongestants and asthma inhalers, energy drinks, some pre-workout supplements, ADHD medications.
- Alcohol — both during drinking and the morning after.
- Sleep deprivation.
- Anxiety and panic. The autonomic nervous system can both produce extra beats and make us much more aware of normal ones. Anxiety and palpitations often feed each other.
- Thyroid overactivity.
- Anemia.
- Dehydration and electrolyte shifts.
- Hormonal changes — pregnancy, menstrual cycle, perimenopause.
When palpitations matter more
Most palpitations are nothing more than a nuisance. We look harder when they:
- Cause fainting or near-fainting.
- Are associated with chest pain or significant shortness of breath.
- Happen in someone with known heart disease, a reduced ejection fraction, or prior cardiac surgery.
- Have a family history of sudden cardiac death or known inherited arrhythmia syndromes.
- Are sustained for many minutes at a fast rate.
- Wake you up from sleep with significant symptoms.
None of these alone makes palpitations dangerous — they just lower the threshold for closer investigation.
How monitoring works
The single most useful piece of data we can get is a tracing during a symptomatic episode. The challenge is matching the duration of monitoring to how often episodes happen.
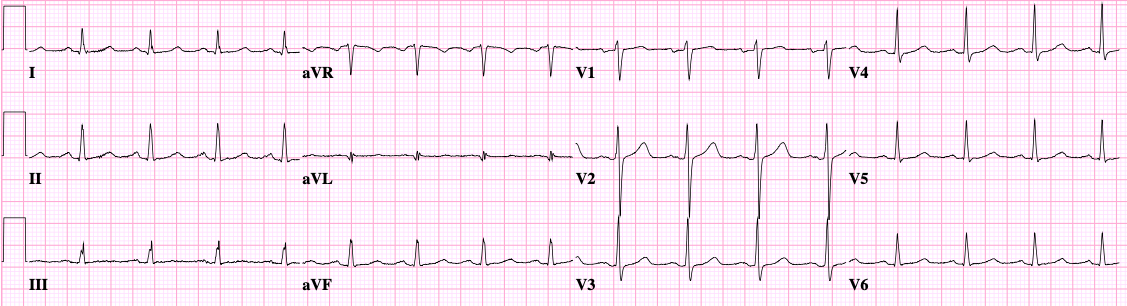
12-lead ECG
A 10-second snapshot. Perfect if you’re symptomatic in the office or emergency room; useless if you’re not.
Holter monitor
A wired monitor worn for 24–48 hours. Best when episodes happen daily.
Patch monitor
A discreet adhesive patch worn on the chest for 1–2 weeks (sometimes longer). The patient presses a button when they feel symptoms, and we correlate symptoms with rhythm afterward. This is now our default for most patients with intermittent palpitations.
Mobile cardiac telemetry (MCT)
Similar form factor to a patch, but transmits in real time and triggers alerts for significant abnormalities.
Implantable loop recorder (ILR)
A small device placed just under the skin of the chest, designed to monitor for up to three years. Used when episodes are rare but important — for example, palpitations associated with fainting.
Smartwatches and consumer ECGs
Increasingly excellent. A patient who can pull out a watch the moment symptoms start and capture a 30-second tracing is doing exactly what a monitor would do. We routinely review smartwatch ECGs in clinic. They are not perfect, but they are a real diagnostic asset.
How we treat palpitations
The plan follows the rhythm we identify.
- No arrhythmia found despite good monitoring during symptoms — strong reassurance, attention to triggers, and often a noticeable reduction in symptoms once the patient knows nothing dangerous is happening.
- PACs / PVCs — usually no treatment beyond addressing triggers. Beta-blockers help when symptoms are bothersome. For very frequent PVCs, ablation can be highly effective.
- SVT — daily medication or, more definitively, catheter ablation.
- AFib — a separate, structured plan covering stroke prevention, rate control, and (often) rhythm control.
- VT or other concerning ventricular arrhythmia — urgent and individualized.
What to expect at your visit
We’ll spend time on the description: when they happen, how long they last, how they start and stop, what makes them better or worse, and what (if anything) you’ve captured on a watch or monitor. We’ll go through medications, stimulants, sleep, and stressors. We’ll review your ECG, often your echocardiogram, and any prior tracings. Then we’ll pick a monitor that fits how often your episodes occur — and from there, the plan usually becomes clear.
Further reading
General-arrhythmia resources from the American Heart Association:
- What Is an Arrhythmia? — AHA Answers by Heart — a two-page plain-English overview of bradycardia, tachycardia, how rhythm problems are diagnosed, and the major treatment options
- Arrhythmias — AHA animation library — pick “Arrhythmias” from the topic menu for an animated walkthrough of the normal electrical system and how rhythm disturbances develop