What is happening in the heart
“Supraventricular” simply means “above the ventricles.” SVT is an umbrella term for fast heart rhythms whose engine sits in the atria or in the small electrical junction between the atria and ventricles — not in the ventricles themselves. During an episode, the heart rate often jumps to 150–220 beats per minute and stays there until the rhythm breaks.
The three patterns we see most often look similar to a patient but use different wiring inside the heart:
AVNRT (AV nodal reentrant tachycardia)
The most common form. Two pathways with slightly different conduction speeds exist inside the AV node — the small junction between the atria and the ventricles. Under the right conditions, the electrical signal loops back on itself inside that junction, going around and around at high speed and driving the rest of the heart along with it.
AVRT (AV reentrant tachycardia)
This form uses an accessory pathway — an extra strand of muscle that someone is born with, connecting the atria and the ventricles outside the normal AV node. The circuit loops between the two chambers using that extra connection. Wolff-Parkinson-White syndrome is the best-known example.
Atrial tachycardia
Here a single small spot in the atrium — outside the sinus node — fires rapidly on its own and drives the heart, like a second engine running too fast.
Why it matters
For most patients, SVT is uncomfortable but not dangerous. The chambers are still filling and emptying in sequence, and the heart muscle itself is healthy. The bigger problems are quality of life and unpredictability — episodes can interrupt work, exercise, driving, and sleep, and some patients describe a lingering anxiety between episodes.
There are two situations where we treat SVT more urgently:
- Long episodes that drop blood pressure or cause chest pain, severe shortness of breath, or fainting.
- AVRT with rapid AFib through an accessory pathway — uncommon, but the reason we take Wolff-Parkinson-White seriously even when symptoms are mild.
How we diagnose it
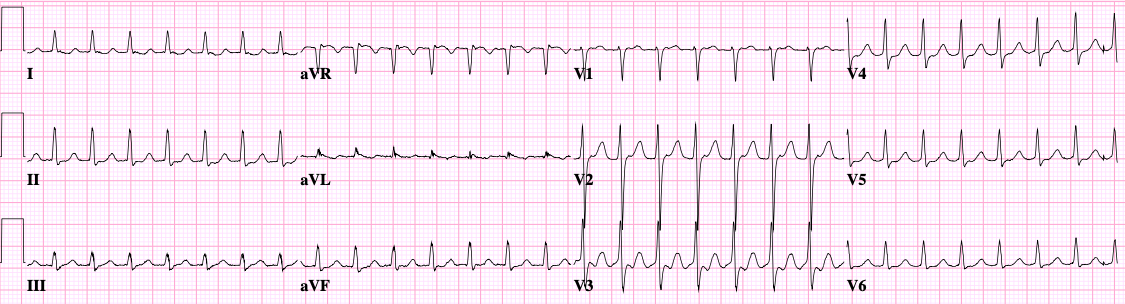
The single most useful piece of information is a 12-lead ECG captured during an episode. The pattern on that tracing usually tells us which type of SVT is at work. Because episodes are often brief, we lean on monitors:
- Holter (24–48 hours) when episodes are frequent.
- Patch monitor (1–2 weeks) when episodes are weekly or so.
- Mobile cardiac telemetry for longer monitoring with real-time review.
- Implantable loop recorder for very infrequent but disabling episodes.
- Smartwatch ECG — increasingly useful for capturing a tracing the moment symptoms hit.
When the diagnosis is still unclear, or when we are planning ablation, we recommend an electrophysiology (EP) study: thin catheters are positioned in the heart through veins in the groin, and we deliberately bring on the rhythm in a controlled setting to map exactly what’s happening.
How we treat it
Stopping an episode
- Vagal maneuvers — bearing down as if having a bowel movement, or applying a cold pack to the face. These work by stimulating the vagus nerve, which briefly slows conduction through the AV node and can break the circuit.
- Adenosine — a short-acting medication given through an IV that interrupts conduction through the AV node for a few seconds. Effective, but the few seconds while it works can feel unpleasant.
- Cardioversion — a brief electrical reset, reserved for episodes that don’t break with medication or that cause significant symptoms.
Preventing future episodes
- Daily medication — beta-blockers or calcium channel blockers reduce how often episodes occur, though they rarely eliminate them.
- Catheter ablation — the definitive treatment for most SVTs. We map the circuit in the EP lab and then create a tiny area of scar that interrupts it. For AVNRT, success rates exceed 95% with a very low complication rate. For most accessory-pathway SVTs, success is similarly high. For atrial tachycardia, success depends on where the focus sits but is generally 80–90%.
What to expect at your visit
We’ll go through what your episodes feel like, how they start and stop, what triggers them, and what (if anything) helps. We’ll review any tracings you’ve captured — from monitors, hospital visits, or your watch. If we already have an ECG during an episode, we can often predict the type. If not, we’ll talk about which monitor makes sense, and whether an EP study with possible ablation is the right next step.