What is happening in the heart
A normal heartbeat starts at the top of the heart and travels down through the wiring system to the ventricles in a tightly orchestrated wave. In ventricular tachycardia, the rhythm bypasses that wiring entirely and fires from somewhere inside the ventricular muscle itself — usually 150 to 250 beats per minute. Because the signal is no longer coming through the normal pathway, the two ventricles squeeze inefficiently and out of sync with the atria. Blood pressure can fall, and if the rhythm degenerates further into ventricular fibrillation, the heart stops pumping altogether. That is what we mean by sudden cardiac arrest.
The two shapes we look for
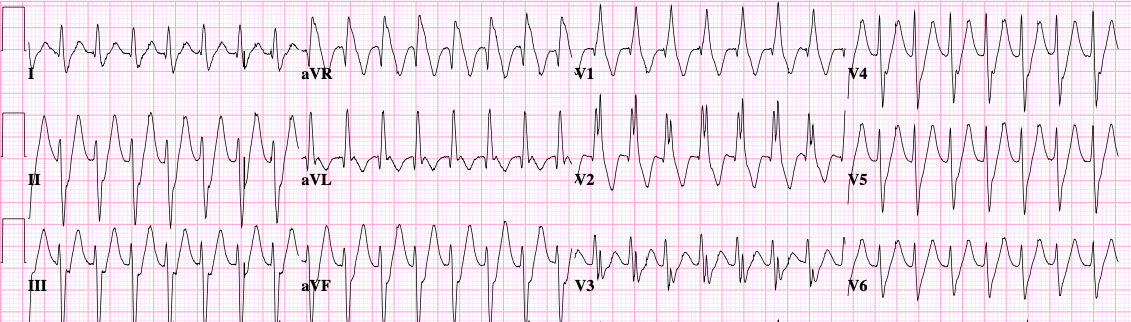
On the ECG, every VT beat looks the same in monomorphic VT — meaning the rhythm is escaping from a single spot in the ventricle and following the same path each time. In polymorphic VT, the QRS complexes change shape from beat to beat, often spiraling, because the rhythm is moving around constantly. The distinction matters because each shape points to different causes and different treatments.
Two big categories of cause
Idiopathic VT — a structurally normal heart
Some patients develop VT despite having a completely healthy heart muscle. These rhythms often arise from very specific spots — the right ventricular outflow tract or one of the fascicles of the left bundle branch are classic locations. Idiopathic VT is usually monomorphic, often triggered by exercise or stress, and is generally well tolerated. The good news is that ablation cures most of these cases.
Scar-mediated VT — VT in a damaged heart
Far more concerning. When heart muscle has been injured — usually by a prior heart attack, but also by cardiomyopathies, sarcoidosis, myocarditis, or surgical scars — strands of surviving tissue weave through the scar. Electrical signals can loop around those strands, creating a sustained, organized circuit. Scar-mediated VT tends to be faster, less tolerated, and is the rhythm we worry about most in patients with reduced ejection fraction.
Polymorphic VT and torsades
When VT is polymorphic, the cause is usually different again — acute ischemia (an unfolding heart attack), severe electrolyte abnormalities, or a long QT interval. Torsades de pointes is a specific polymorphic VT seen with long QT and is covered in the long-QT entry.
Why it matters
VT is the most common mechanism of sudden cardiac death in adults. Even when an episode self-terminates, it’s a warning shot. We take every documented VT seriously, work hard to find the underlying cause, and decide whether an ICD is needed.
How we diagnose it
We rely on the 12-lead ECG captured during an episode whenever possible — the shape and rate of the rhythm tell us where it’s coming from. When VT is intermittent, we use longer monitors: patch monitors, mobile telemetry, or a loop recorder. We then look at the heart itself — usually with an echocardiogram, often with a cardiac MRI to look for scar — to decide which category of VT we’re dealing with. In selected cases, we do an electrophysiology study: catheters inside the heart that map the circuit directly.
How we treat it
Treatment has three pillars, and most patients need more than one.
- Treat what’s underneath. Open a blocked artery, optimize heart-failure medications, correct potassium and magnesium, stop a QT-prolonging drug. Many VT problems improve dramatically once the trigger is addressed.
- Suppress the rhythm. Beta-blockers are the foundation for almost every type of VT. Antiarrhythmic drugs — amiodarone, sotalol, mexiletine — are added when needed.
- Ablation. For idiopathic VT, ablation is often curative. For scar-mediated VT, ablation reduces the burden of episodes and shocks; we map the scar and burn the circuits that drive the rhythm.
ICDs: primary and secondary prevention
An implantable cardioverter defibrillator is the only therapy proven to abort a sudden-cardiac-death event in progress. We use them in two settings:
- Secondary prevention — you’ve already had a sustained VT or a cardiac arrest. The ICD is highly recommended in nearly every case.
- Primary prevention — you haven’t had an event, but your risk is high enough that we recommend the device before something happens. The clearest example is a reduced ejection fraction (typically 35% or below) despite good medical therapy. Inherited conditions like hypertrophic cardiomyopathy, long QT, and Brugada have their own risk frameworks.
ICDs come in transvenous and subcutaneous designs, and the choice depends on whether you also need pacing.
What to expect at your visit
We’ll go through the ECG of your episode (or any monitor recordings), look at your heart’s structure and function, and figure out which category of VT you’re in. From there we talk through medication, ablation, and ICD options. None of these decisions are made in isolation — they’re based on the underlying cause, your symptoms, your other medical conditions, and your goals.